Historic intersex rights inquiry in Senate
Image: The intersex pride flag.
A REPORT into intersex health, sterilisation and rights and its recommendations that was discussed in the Senate last night has become the first of its kind to be discussed in Federal Parliament.
In the course of 30 minutes, senators from all three major political parties spoke about intersex health issues to mark World Health Day in light of what is the first-ever parliamentary inquiry into intersex health and rights.
Western Australian Greens Senator Rachel Siewert spoke as Chair of the Community Affairs References Committee, which published the Involuntary or Coerced Sterilisation of Intersex People in Australia report last October.
Meanwhile, Queensland Coalition Senator Sue Boyce spoke as chair of the Community Affairs Legislation Committee, while Queensland Labor Senator Claire Moore spoke as a former member of the committee enquiry.
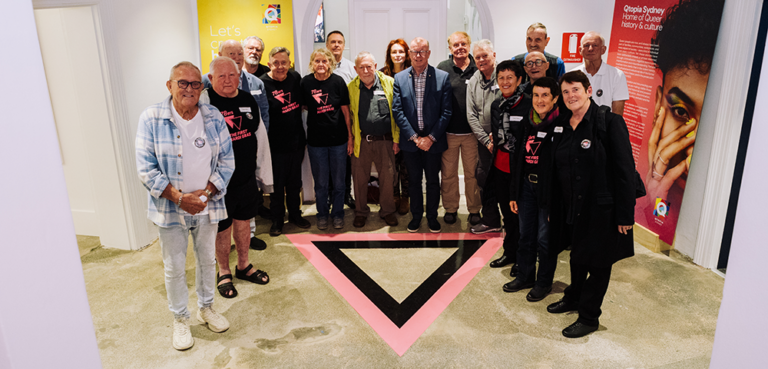
Organisation Intersex International (OII) Australia representatives were present in the gallery during the historic discussion and welcomed the occasion.
OII president Morgan Carpenter said: “In three extraordinary and powerful speeches we heard clear recognition that the medical treatment of intersex people is a human rights issue, that intersex is not a disorder, and that intersex people must be heard.
“Our issues are simply when regarded as issues of bodily autonomy, human rights, and individual choice of expression. Alone these statements are momentous, but the Senators also told some of our personal stories, and paid tribute to members of intersex-led organisations, OII Australia and the AIS Support Group Australia.
“We are enormously excited by today’s cross-party speeches. We hope that they will promote a better understanding of our health and human rights concerns, and policy changes that will lead to better health outcomes.”
OII vice president Tony Briffa echoed Carpenter’s sentiments.
“This is a turning point in the way that intersex people in Australia are seen and treated,” Briffa said.
“We have long fought for our voices to be heard, so to have the Australian Parliament acknowledge our existence and our issues – as discussed in detail in the Senate report – is vital.
“Today heralds a moment in our movement where our politicians were united in expressing great concern about the current paradigm. It’s not okay to pathologise us. We thank the Senators for today’s speeches, and we look forward to the implementation of the Senate Report Recommendations.”
In her speech, Senator Siewert spoke about the disordering of intersex, and the nature of intersex differences.
“I think most people in the community do not understand ‘intersex’ and do not understand the issues. People in the past have seen it as a disorder — in fact, I think it is fair to say that many still do,” she said.
“So one of our recommendations is that terms such as ‘disorder’ should not be used. We strongly recommend that government and other organisations use the term ‘intersex’, and do not use the term ‘disorders of sexual development’, because intersex people should not be seen to have a disorder.
“We also point out that there is no single condition that is intersex. There are in fact 30 or 40 testable genetic, anatomical and hormonal types of sex difference. We need to make sure that that is clear.
“Most importantly, we need to understand that this is a human rights issue.”
Senator Sue Boyce commented on the origins of the inquiry, and how it grew out of an inquiry into the involuntary or coerced sterilisation of people with disabilities – with many similar issues encountered.
“The issues that were similar were issues where some in the medical profession thought they knew better than anyone else; they would make decisions not only on behalf of individuals but on behalf of families as to what gender might be assigned to a baby or to a young child when this was not immediately obvious,” she said.
“What differed was the fact that the people with disabilities that we were talking about in many cases were seen as unable to give informed consent because of cognitive impairment. In the case of intersex people, the main issue was that this was being done when they were too young to give consent.”
Meanwhile, Senator Moore commented on the issues of stigma, respect, and ignorance: “We heard consistently about the issues of medicalisation. When looking at the history of intersex, we consistently see that it has been defined in a medical way.
“As Senator Boyce put it, the political focus has meant that people are ignored to a large extent and are looked upon as ‘case load’, as things that have treatment rather than people with feelings and human rights. In our recommendations we have consistently said that the issues around intersex in our country should be seen as human rights issues so that people have support, recognition and respect.
“The clear message from our report is that people should be valued and respected. They know who they are and they should be able to share that openly with all of us.”
THE RECOMMENDATIONS:
1) The committee recommends that governments and other organisations use the term ‘intersex’ and not use the term ‘disorders of sexual development’.
2) The committee recommends that health professionals and health organisations review their use of the term ‘disorders of sexual development’, seeking to confine it to appropriate clinical contexts, and should use the terms ‘intersex’ or ‘differences of sexual development’ where it is intended to encompass genetic or phenotypic variations that do not necessarily require medical intervention in order to prevent harm to physical health.
3) The committee recommends that all medical treatment of intersex people take place under guidelines that ensure treatment is managed by multidisciplinary teams within a human rights framework. The guidelines should favour deferral of normalising treatment until the person can give fully informed consent, and seek to minimise surgical intervention on infants undertaken for primarily psychosocial reasons.
4) The committee recommends that the Commonwealth government provide funding to ensure that multidisciplinary teams are established for intersex medical care that have dedicated coordination, record-keeping and research support capacity, and comprehensive membership from the various medical and non-medical specialisms. All intersex people should have access to a multidisciplinary team.
5) In light of the complex and contentious nature of the medical treatment of intersex people who are unable to make decisions for their own treatment, the committee recommends that oversight of these decisions is required.
6) The committee recommends that all proposed intersex medical interventions for children and adults without the capacity to consent require authorisation from a civil and administrative tribunal or the Family Court.
7) The committee recommends that the Standing Committee on Law and Justice consider the most expedient way to give all civil and administrative tribunals in all States and Territories concurrent jurisdiction with the Family Court to determine authorisation for intersex medical interventions proposed for a child.
8) The committee recommends that civil and administrative tribunals be adequately funded and resourced to consider every intersex medical intervention proposed for a child.
9) The committee recommends that the special medical procedures advisory committee draft guidelines for the treatment of common intersex conditions based on medical management, ethical, human rights and legal principles. These guidelines should be reviewed on an annual basis.
10) The committee recommends that complex intersex medical interventions be referred to the special medical procedures advisory committee for consideration and report to whichever body is considering the case.
11) The committee recommends that the provision of information about intersex support groups to both parents/families and the patient be a mandatory part of the health care management of intersex cases.
12) The committee recommends that intersex support groups be core funded to provide support and information to patients, parents, families and health professionals in all intersex cases.
13) The committee recommends that the Commonwealth Government support the establishment of an intersex patient registry and directly fund research that includes a long-term prospective study of clinical outcomes for intersex patients.
14) The committee recommends that the Commonwealth government investigate the appropriate regulation of the use of dexamethasone for prenatal treatment of CAH.
15) The committee recommends that, effective immediately, the administration of dexamethasone for prenatal treatment of CAH only take place as part of research projects that have ethics approval and patient follow-up protocols.